
Are you hiding your legs despite reaching your goal weight because of Ozempic Thighs? You are not alone; rapid weight loss often outpaces your skin’s elasticity, leading to Ozempic legs with noticeably saggy inner thighs and crepey texture. Understanding that diet and exercise alone cannot fix loose skin, this article from Tran Plastic Surgery provides information on advanced thigh contouring solutions specifically designed to eliminate this “empty shell” and reveal the toned legs you have worked so hard to build.
1. What Are Ozempic Thighs (Ozempic Leg)?
Ozempic thighs, also known as Ozempic legs or Wegovy legs, is a non-medical term increasingly recognized to describe the characteristic aesthetic decline of the thighs following rapid semaglutide-induced weight loss. In the context of reconstructive and post-weight-loss body contouring, this condition reflects a triad of severe skin laxity, subcutaneous fat depletion, and GLP-1-associated muscle atrophy.
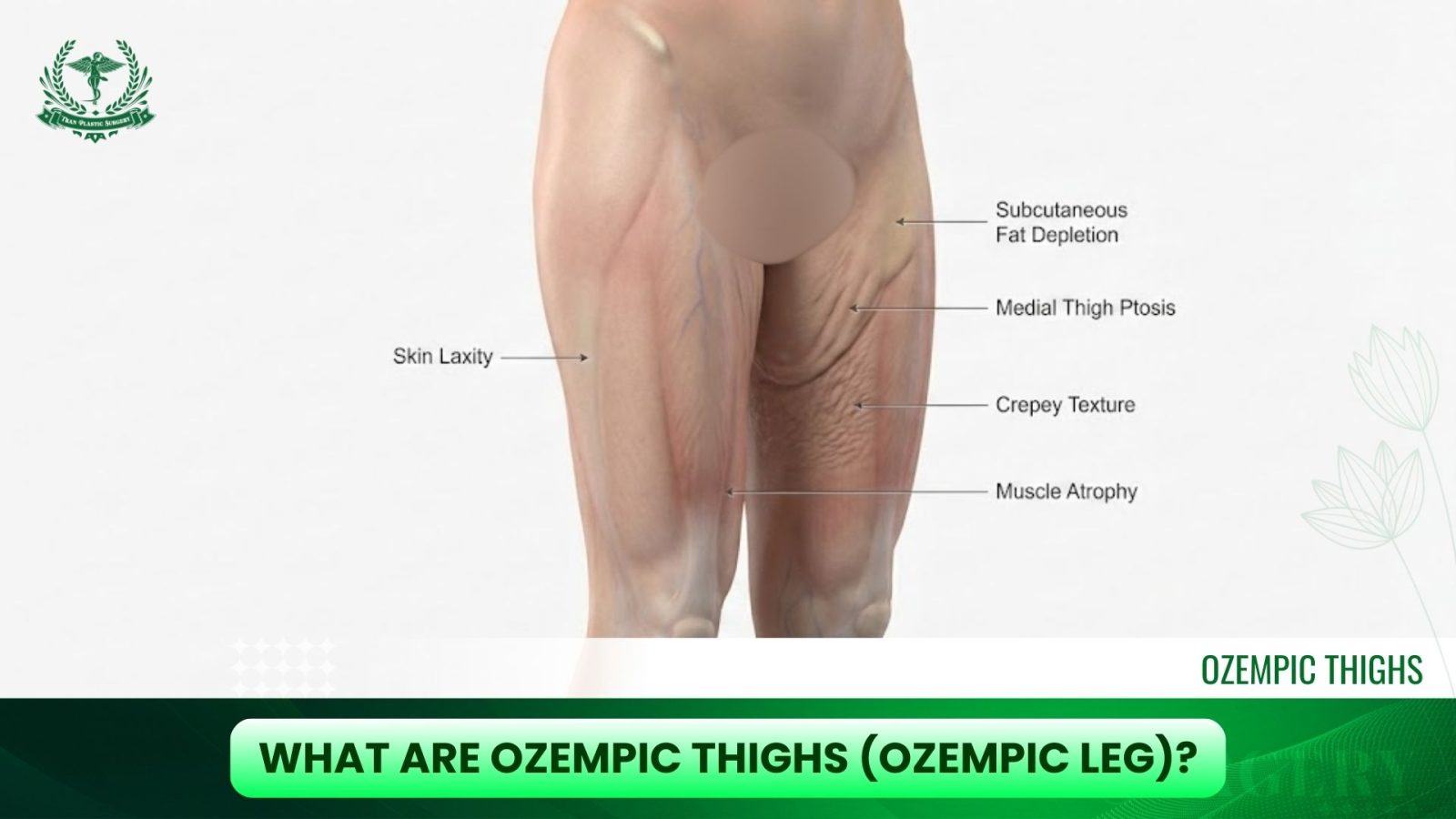
Unlike gradual weight reduction, the accelerated metabolic shift triggered by GLP-1 receptor agonists outpaces the skin’s ability to retract. As a result, patients often develop a visibly deflated thigh contour, medial soft-tissue ptosis (drooping of the inner thighs), and diffuse textural irregularities such as crepey skin or the mottled appearance sometimes described as strawberry legs. These changes are functionally and aesthetically significant and often require a reconstructive approach similar to traditional massive-weight-loss deformities.
2. Recognizing Symptoms of Ozempic Thighs and Loose Skin
Patients presenting with Ozempic thighs typically exhibit a particular pattern of physical changes that distinguishes this condition from routine post-weight-loss skin laxity.
2.1. Saggy Inner Thighs
Marked medial thigh redundancy creates an empty-envelope effect, in which the skin hangs without sufficient underlying volume or structural support. This is one of the most defining manifestations of Ozempic-related thigh laxity.

2.2. Ozempic Muscle-Wasting Legs
The catabolic effects of rapid GLP-1-induced weight loss lead to quadriceps and adductor muscle depletion, producing a frail, flattened leg profile rather than the expected toned appearance. This muscle wasting is a major contributor to overall thigh deflation.

2.3. Textural and Dermal Changes
Patients frequently report crepey skin on the knees, thinning of the dermis, and the strawberry legs appearance. These issues stem from dehydration, collagen loss, and reduced subcutaneous cushioning.

2.4. Physical Discomfort
Beyond cosmetic concerns, loose thigh skin can cause functional challenges such as chafing, recurring rashes (intertrigo), moisture trapping, and difficulty achieving a proper fit in clothing. These symptoms are common indications for post–semaglutide body contouring or thigh lift surgery.

>>> You might want to read this:
3. Pathophysiology of Ozempic Thighs: Fat Loss vs. Muscle Wasting
For patients searching terms such as Ozempic muscle wasting legs, saggy inner thighs, or Ozempic loose skin thighs, the underlying concern is the same: a profound structural change in the thigh anatomy caused by rapid GLP-1–mediated weight reduction. Understanding the pathophysiology requires examining both the loss of adipose tissue volume and the parallel decline in lean muscle mass, which together produce the hallmark “deflated” thigh appearance associated with Ozempic thighs.
3.1 Why Ozempic Thighs Occur? The Mechanism of Rapid Deflation
Semaglutide acts as a GLP-1 receptor agonist, suppressing appetite, reducing caloric intake, and accelerating weight loss to a degree that often surpasses physiological adaptation. When energy expenditure exceeds intake, the body shifts into a catabolic state, breaking down not only stored fat but also essential lean tissue.
In the thighs, the rapid depletion of the subcutaneous fat pad eliminates the natural tension that keeps the skin taut and supports the thigh contour. As this structural cushion collapses, patients develop the classic Ozempic loose skin thighs, characterized by wrinkling, medial thigh drooping, and loss of smooth surface texture. Unlike gradual weight loss, the rapid rate of semaglutide-induced weight loss prevents the dermis from producing enough collagen and elastin to recoil effectively.

3.2 Ozempic Muscle Wasting Legs and Sarcopenia
One of the most defining contributors to the Ozempic thigh deformity is sarcopenia, or the reduction of skeletal muscle mass. Clinical findings indicate that up to 40% of semaglutide-related weight loss may come from lean tissue, significantly affecting leg aesthetics.
a. Structural Collapse
The quadriceps, hamstrings, and adductor groups act as the primary scaffolding system for the overlying soft tissue. When these muscles atrophy, the thigh loses its volume, firmness, and external contour. This “internal collapse” magnifies the appearance of loose skin on the legs, regardless of the patient’s overall weight-loss success.
b. Metabolic Impact
Rapid muscle loss also contributes to the “skinny fat” metabolic profile seen in many GLP-1 patients, where the body becomes lighter but structurally weaker. In this state, exercise alone cannot restore the tension between skin, fascia, and deeper tissues, because once the skin-fascia interface has been overstretched, it rarely contracts back to its original form. This is why so many patients ultimately seek leg contouring, thigh lift surgery, or post–Ozempic body reconstruction.
3.3 The “Empty Envelope”: Why Exercise Cannot Tighten Thigh Skin
Searches such as “How to tighten thigh skin” often misunderstand a key anatomical principle: the relationship between the superficial fascial system (SFS) and the soft tissue it supports. After rapid weight loss, the SFS becomes permanently lengthened, while the volume of thigh muscle and fat shrinks dramatically.
This creates the classic “empty envelope” deformity, in which the “contents” (fat and muscle) no longer fill out the “envelope” (skin). No amount of strength training can reverse structural overstretching once the collagen matrix has failed. In these cases, mechanical excision, such as a medial thigh lift, often is the only definitive solution for correcting saggy inner thighs and achieving meaningful contour restoration.
4. Surgical Treatments for Ozempic Thighs
Significant weight reduction caused by GLP-1 medications such as Ozempic or Wegovy often results in loss of adipose volume in the thighs, accompanied by skin laxity, contour irregularities, and reduced structural support of the soft tissues. When nonsurgical interventions cannot adequately restore shape or firmness, surgical procedures offer more precise correction. These options focus on repositioning tissue, removing redundancy, and re-establishing proportional contour between the hip, thigh, and lower leg.
4.1. Thigh Lift (Thighplasty)

A thigh lift is the most direct method for addressing excess skin and structural sagging. It is especially effective for patients who have experienced rapid or massive weight loss and are left with deflated, wrinkled inner thighs that do not respond to exercise.
How it works:
- The surgeon creates incisions along the groin crease or vertically along the inner thigh, depending on the degree of laxity.
- Redundant skin is excised, and the underlying tissue is reshaped to improve firmness.
- Soft-tissue suspension techniques are used to secure the lifted contour and prevent downward migration over time.
Ideal for:
- Severe skin redundancy
- Thighs with a “collapsed” appearance after semaglutide-induced weight loss
- Patients wanting long-term correction rather than subtle enhancement
4.2. Liposuction for Residual Fat Pockets
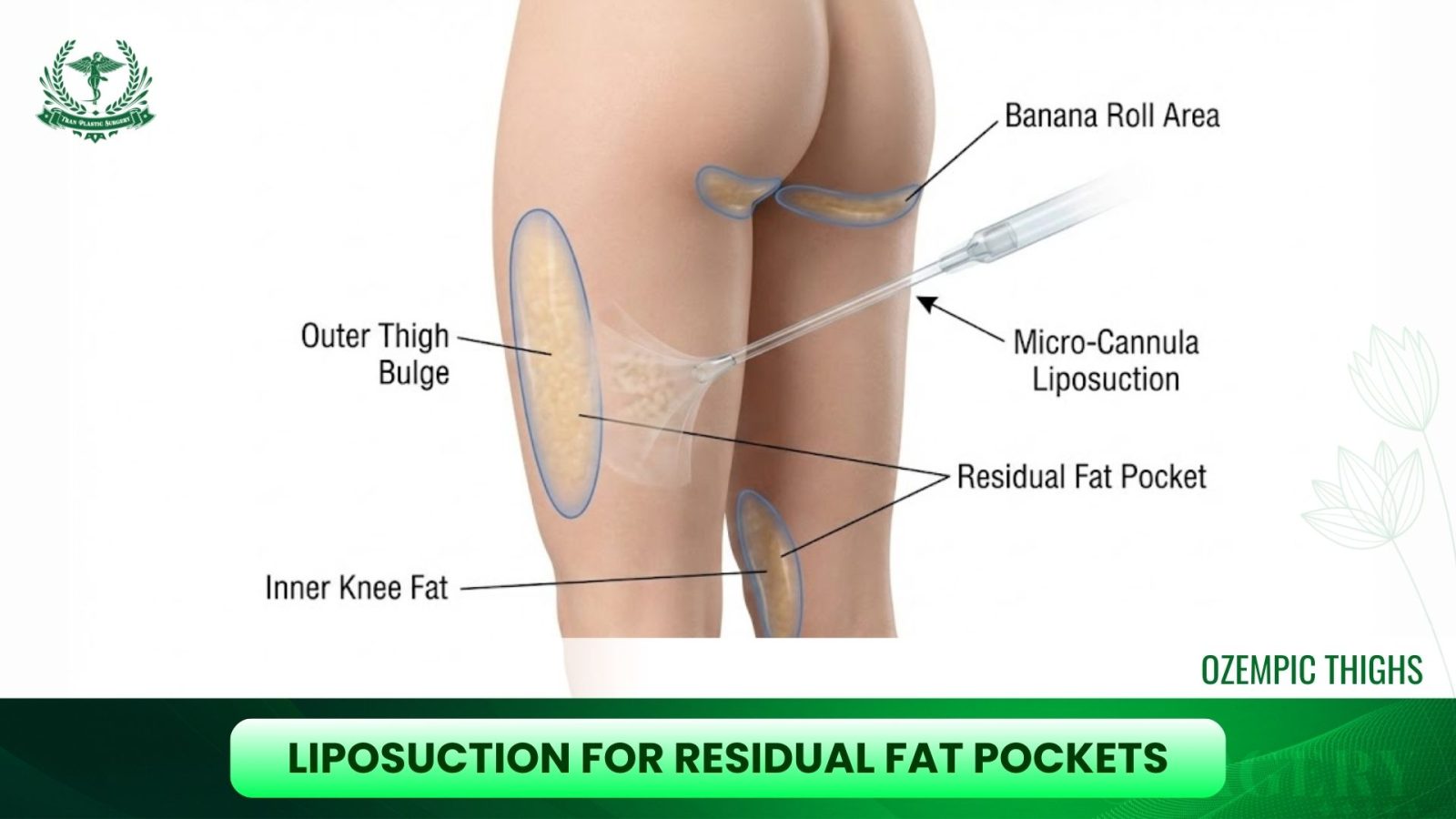
Not all patients lose fat evenly throughout the thighs. Some develop disproportionate pockets of fat around the inner knee, outer thigh, or the “banana roll” crease under the buttocks. Liposuction works well when the primary issue is contour imbalance rather than skin excess.
How it works:
- Small cannulas remove localized adipose deposits through tiny incisions.
- The aim is to restore a balanced silhouette without over-reducing volume, which could worsen the hollowed look created by GLP-1 therapy.
Ideal for:
- Patients with mild to moderate excess fat
- Individuals with good skin elasticity or those combining liposuction with a skin-tightening procedure
4.3. Fat Transfer to Restore Volume
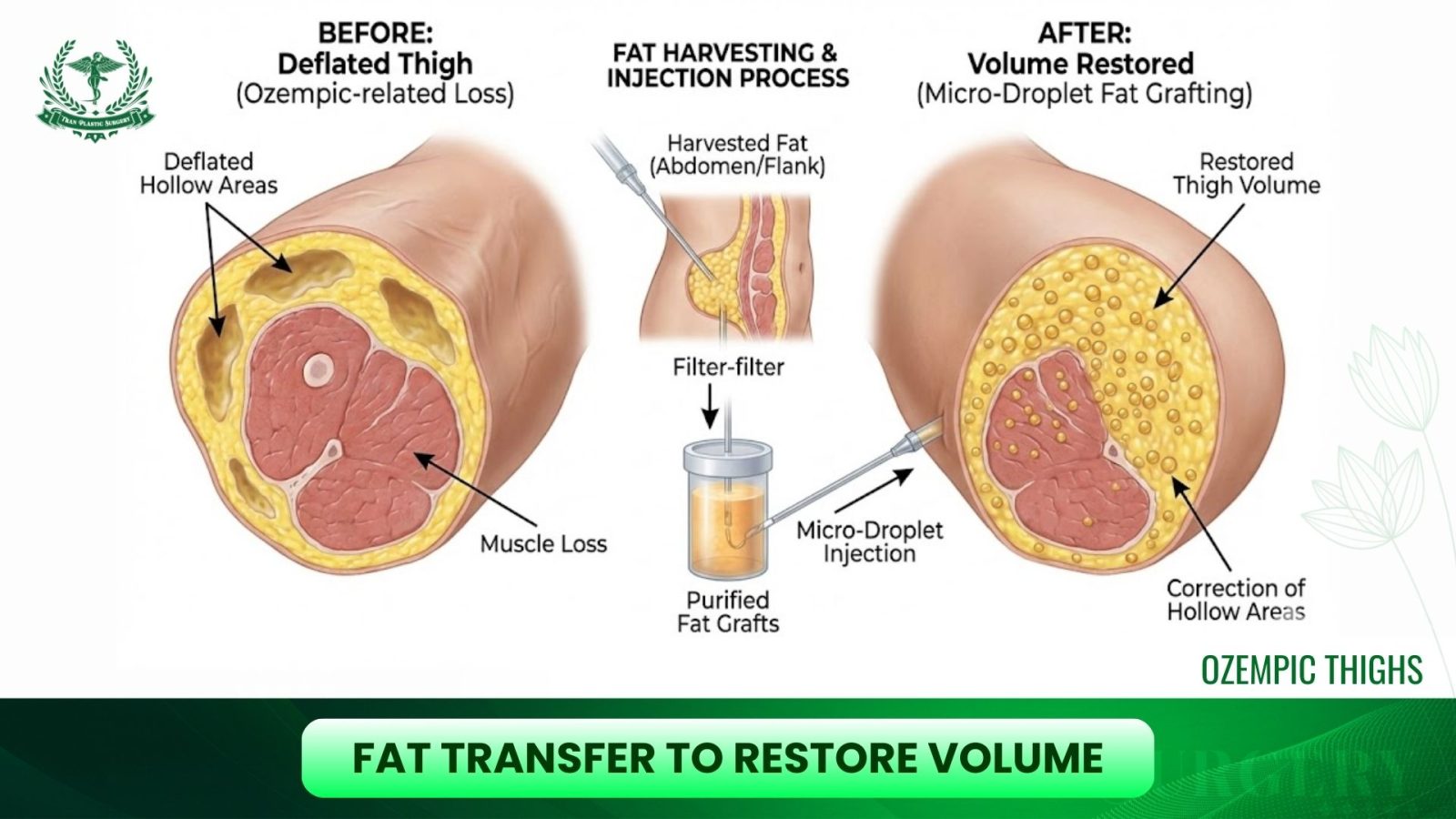
In cases where Ozempic leads to over-deflation of the thighs, producing a “stringy” or prematurely aged appearance, fat transfer can selectively restore lost volume.
How it works:
- Fat is harvested from another area of the body through liposuction.
- The purified fat is injected into strategic zones of the thighs to improve curvature, fill hollows, and re-establish natural proportions.
- This method offers a more natural feel than implants and is ideal when added volume is needed rather than when tissue removal is required.
Ideal for:
- Visible hollows on the inner or outer thighs
- Patients with asymmetry caused by uneven weight loss
- Thin patients seeking subtle, natural
4.4. Combination Thigh Contouring
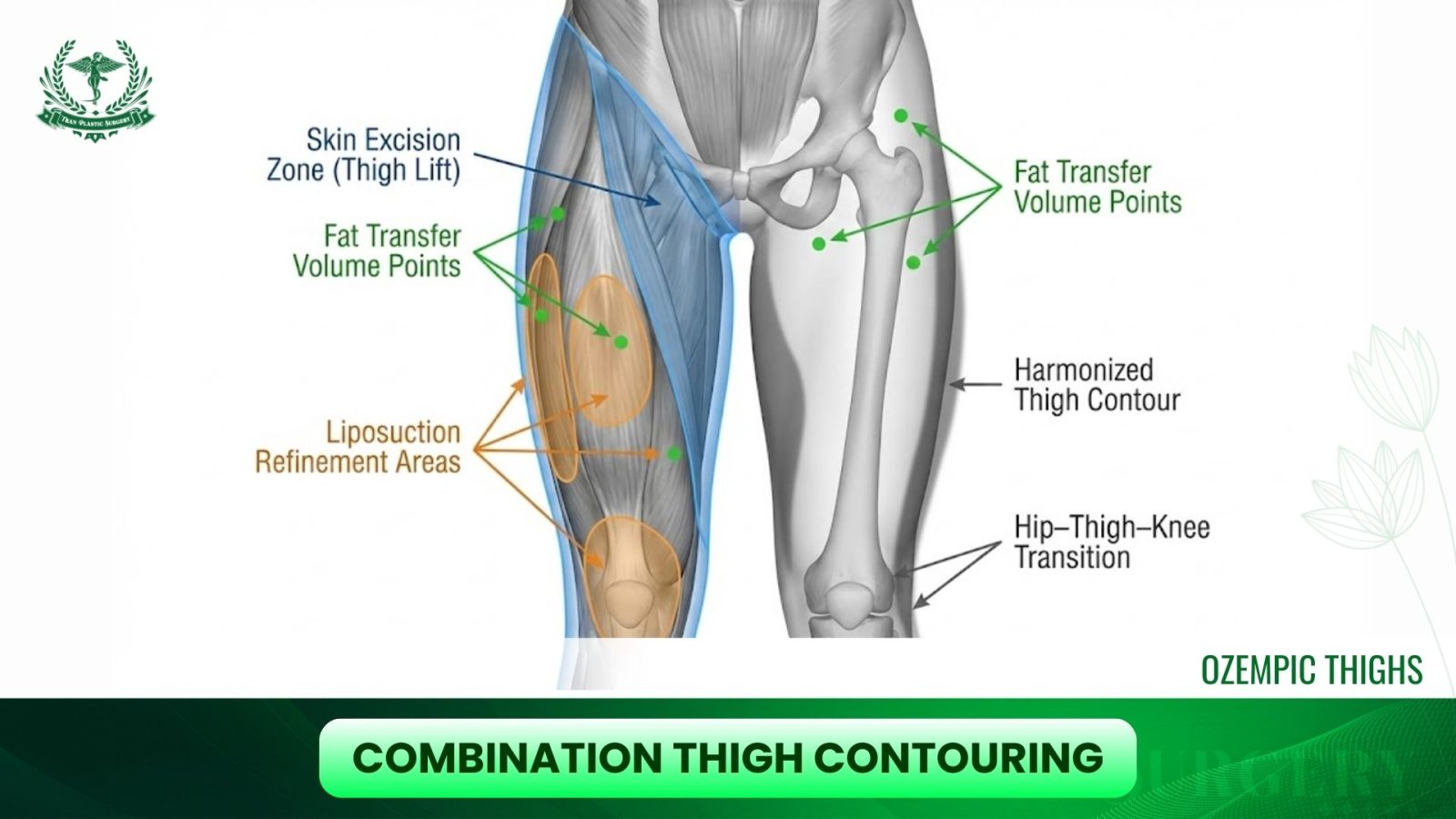
Many individuals require a combined approach because Ozempic-related changes are multifactorial, and loose skin, deflated tissue, and small pockets of remaining fat often coexist.
A combined surgical plan may include:
- Thigh lift to remove redundant skin
- Liposuction to fine-tune shape
- Fat transfer to correct irregularities or restore natural curves
Integrated procedures are designed to harmonize the thigh contour from hip to knee and create a smoother transition into the buttocks and calves.
At Tran Plastic Surgery, Dr. Tuan Tran specializes in post–weight loss body contouring and offers advanced solutions for severe thigh laxity, including medial, vertical, and spiral thigh lifts. Patients receive personalized treatment plans, meticulous surgical care, and supportive follow-up to help them achieve smoother, firmer, and more balanced leg contours.

5. Non-Surgical Solutions for Ozempic Thighs and Loose Skin
Not every patient who experiences thigh changes after GLP-1–associated weight loss is ready for surgery. Many prefer to explore non-invasive or minimally invasive methods that improve skin tone, reinforce the soft-tissue framework, or address early signs of muscle atrophy. While these approaches cannot match the precision of surgical contouring, they can meaningfully improve firmness, texture, and overall leg aesthetics when used appropriately.
5.1 Energy-Based Devices for Thigh and Leg Contouring
Energy-based tissue tightening has become a key option for individuals with moderate laxity who do not have the severe redundancy that would require excisional surgery. These devices work by heating the dermis and the fibroepithelial network, triggering collagen remodeling and gradually tightening the skin.
a. BodyTite (RFAL – Radiofrequency-Assisted Lipolysis)
BodyTite is a minimally invasive device that delivers bipolar radiofrequency energy beneath the skin. By directly heating the fibroseptal network, it contracts supportive septal fibers and stimulates deep collagen production.
b. Renuvion (Helium Plasma Radiofrequency)
Renuvion delivers a combination of cold helium plasma and radiofrequency energy to rapidly heat the skin’s underside while limiting thermal damage to surrounding tissues.

5.2 Addressing Thigh Muscle Atrophy Without Surgery
A significant number of patients on GLP-1 medications report not only fat loss but also reductions in muscle mass, especially in the quadriceps and hamstrings. When muscle volume decreases, the overlying skin appears looser, and the overall leg contour looks less supported. Managing this requires more than surface-level tightening—it involves rebuilding the structural framework beneath the skin.
a. Muscle Stimulation and Conditioning Technologies
Devices such as Emsculpt NEO combine high-intensity focused electromagnetic (HIFEM) stimulation with radiofrequency heating to promote muscle hypertrophy while also inducing mild fat reduction.
b. The Rebuilding-the-Scaffold Approach
For patients experiencing both loose skin and muscle atrophy, a staged or combined protocol can offer more balanced improvement:
- Energy-based tightening to improve dermal elasticity
- Muscle stimulation to restore foundation and contour
- Lifestyle recommendations to maintain muscle mass (progressive resistance training, adequate protein intake)
This combined strategy enhances outcomes by addressing both the superficial and deep contributors to thigh aging and deflation.
6. Recovery and Scarring After Thigh Surgery
Recovery after thighplasty, whether medial, vertical, or spira,l requires careful management due to the unique anatomical challenges of the inner thigh. The area is subject to moisture, friction, and constant motion, all of which can influence wound healing and long-term scar quality. Educating patients about these variables is essential for setting realistic expectations.
6.1 Management of Thigh Lift Scars
Thigh lift incisions, particularly those placed in the groin crease, lie in a high-moisture environment. Sweat, friction from walking, and natural skin folds create conditions that may stress wound edges. Because of this, maintaining dryness is a priority during the first one to two weeks. Strategies include:
- Absorbent dressings to wick moisture
- Avoiding prolonged sitting with excessive hip flexion
- Gentle hygiene routines to reduce maceration
- Preventing early stretching of the incision line to avoid wound separation
Vertical thigh lift incisions run along the inner thigh, where the skin is thin and mobile. These require additional attention to avoid tension that could widen the scar.
Scar maturation follows a predictable timeline. Incisions generally appear red or pink for the first several months due to increased vascularity. Over a 9–12 month period, they gradually lighten and soften as collagen reorganizes.
Evidence-based practices for optimal scar refinement include:
- Silicone sheeting or silicone gel, which remains the gold standard for minimizing hypertrophy and improving pliability
- Sun avoidance, as UV exposure can cause hyperpigmentation in the early stages
- Laser therapy, such as fractional non-ablative resurfacing, for patients prone to redness or textural irregularities
With proper care, most groin-incision scars remain discreet, while vertical incisions become less conspicuous over time, even though they remain visible.
6.2 Relief From Thigh Chafing Due to Excess Skin
For many patients who have loose, pendulous thigh skin after rapid weight loss, chronic chafing is a daily issue. Surgical removal of redundant tissue provides almost immediate mechanical relief once swelling subsides, as the soft tissues are no longer rubbing together during walking.
During the initial recovery phase, typically the first four to six weeks, patients wear compression garments continuously. These garments serve several functions:
- Limiting edema
- Reducing dead space to prevent fluid collection
- Supporting newly contoured tissues as they adhere to underlying structures
- Minimizing discomfort during ambulation
By stabilizing the tissues during this period, the contour achieved in surgery is preserved, and long-term skin irritation is significantly reduced.
7. Cost Considerations for Treating Ozempic-Related Thigh Changes
Treatment expenses for post–weight loss thigh concerns vary widely, reflecting differences in anatomy, procedural complexity, and regional market dynamics. Patients should understand the various components that contribute to the total cost.
7.1 Estimated Pricing for Thigh Surgery (2025)
Surgeon’s Professional Fees
Typical ranges are $6,000 to $15,000, depending on:
- The extent of excess skin
- Whether the case involves previous weight-loss surgery
- The need for advanced techniques, such as vertical or spiral lifts
- The surgeon’s expertise in massive-weight-loss body contouring
Facility and Anesthesia Fees
Accredited surgical facilities and board-certified anesthesiologists add $2,000 to $5,000. Longer procedures, such as combining a medial and a vertical lift, may fall at the higher end of this range.
Overall Financial Planning
For a comprehensive thighplasty or lower-extremity skin-reduction procedure, most patients invest $8,000 to $18,000. More complex combined procedures, such as pairing a thigh lift with a lower body lift, may exceed this range.
7.2 Insurance Considerations and Functional Coverage
Thigh lifts performed solely for contouring are considered cosmetic and therefore not reimbursed by insurance. However, select patients may qualify for partial coverage if excess skin is causing functional problems.
Situations that may support an insurance claim include:
- Recurrent fungal or bacterial infections in skin folds
- Documented rashes resistant to conservative treatment
- Skin breakdown or ulceration from chronic friction
- Persistent moisture-associated dermatitis affecting mobility
In such cases, insurers may approve a panniculectomy-style removal of the problematic tissue, though they typically do not cover aesthetic refinement or circumferential sculpting.
Thorough documentation, including photographs, failed treatments, and physician notes, is essential for anyone pursuing functional coverage.
8. In Conclusion
The condition commonly referred to as Ozempic Thighs represents a distinct morphological consequence of rapid, medication-induced weight loss. A comprehensive approach, one that integrates an understanding of soft-tissue biomechanics, dermal quality changes, and post–massive weight loss physiology, is essential for adequate correction. For many patients, surgical interventions such as medial, vertical, or spiral thighplasty provide the only reliable means of restoring anatomical tension and functional contour. At the same time, clear communication about scar behavior, staged treatments, and realistic outcomes remains critical. Thanks for reading the article on Tran Plastic Surgery.


